HIP RESCULPTING
Hip resculpting is a procedure that has been recently advocated for the treatment of hip impingement. Impingement results either because the femoral head (ball) is not quite spherical or because the acetabulum (socket) is too deep; thus when the hip is flexed fully the neck of the femur is pushed against the labrum and acetabulum at the front of the hip, causing damage to these structures.
More recently, Hip Arthroscopy has been used to perform hip resculpting, the advantages being smaller scarring, reduced morbidity and faster recovery. The aim of hip resculpting is to remove some of the bone from the femoral neck to prevent it from causing damage to the labrum, and to allow greater movement – particularly flexion – of the hip. If the labrum has already been damaged it can be repaired or the damaged area removed during the resculpting operation.
The anticipation is that by preventing damage to the labrum and effectively making the femoral head more spherical, the development of osteoarthritis of the hip can be delayed or even prevented.
The long term results of hip resculpting are not known although the early results are encouraging. NICE recommendations state that patients undergoing this procedure should be followed up on a long term basis; results should be properly documented and audited. Hip resculpting is an operation that should only be performed by surgeons with experience of the technique.
INDICATIONS FOR HIP RESCULPTING
There are several indications for undertaking resculpting of the hip:
• Symptomatic femoro-acetabular impingement (with x-ray evidence)
• Normal cartilage (i.e. no evidence of arthritis) – hip arthroscopy may be needed beforehand to prove this
THE PROCEDURE
Hip resculpting surgery involves an inpatient stay of 3-4 days; the patient will generally be admitted the day before the operation. The consultant and anaesthetist will see the patient prior to surgery and the hip undergoing the procedure will be marked.
Hip resculpting is usually performed under a general anaesthetic. There are 2 different surgical approaches (other than the arthroscopic approach) that can be used.
The first involves cutting through the bone on the outer side of the femur (a trochanteric osteotomy) and retracting this segment of bone in order to gain access to the hip joint. The hip is dislocated very carefully and the damaged area of bone on the femoral neck removed. Any labral tears are repaired if possible or removed if they are beyond repair. At the end of the operation the hip is relocated and the cut segment of femoral bone reattached with screws.
The second involves a smaller incision over the front of the hip (the mini-anterior approach). The hip joint can then be opened and the cause of the impingement removed. The labrum can be repaired at the same time.
At the end of the procedure a dressing is applied to the wound. Foot pumps, elastic stockings and occasionally an injection to thin the blood are used to lower the risk of blood clots forming in the legs.
Blood tests and X-rays will be taken in the early post-operative period to ensure that blood levels have not substantially changed and that sufficient bone has been removed.
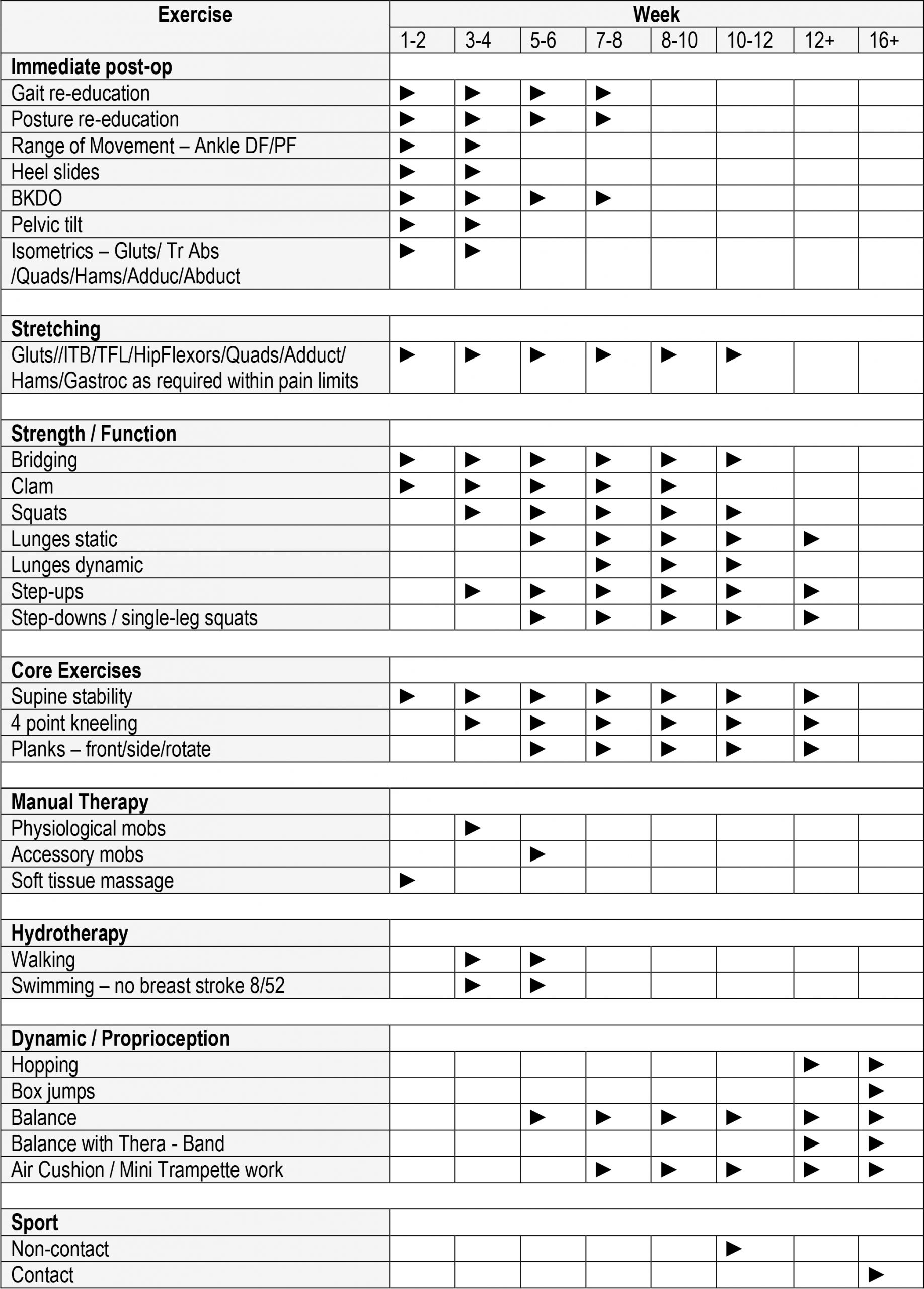
Following surgery patients are given an instruction sheet showing exercises that are helpful in speeding up recovery. This can be seen below:
Complications specific to the operation include:
Persistance of symptoms
Patients may still have hip pain even after adequate resculpting
Progression to osteoarthritis
Whilst resculpting is performed to hopefully reduce the risk of osteoarthritis, there are no guarantees and OA may still develop (usually years) after resculpting
Avascular necrosis of the femoral head
The reported risk of this is very low (< 1%) but if it develops it can have catastrophic implications for the hip; subsequent hip replacement may be necessary.
Non-union of the trochanteric osteotomy
This is where the cut part of the femur fails to unite to the rest of the bone after surgery. Re-operation to re-fix the segment, possibly with the use of a bone graft may be required
Stiffness
Occasionally scarring around the hip causes stiffness. This usually responds well to physiotherapy.
Numbness
Occasionally the nerve that supplies the skin on the outer part of the thigh (called the lateral cutaneous nerve of the thigh) can be stretched during surgery and a numb patch subsequently develops. This usually resolves after 6 months but in rare cases can be permanent.
OUTCOME
The long term outcome of hip resculpting is not yet known. The hope is that it will at least delay if not negate the need for future hip replacement in many patients. Early reports suggest that in the short-term, relief of symptoms is usually achieved.
Discussion with James is important to answer any questions that you may have. For information about any additional conditions not featured within the site, please contact us for more information.
MEET JAMES
QUICK ENQUIRY





